

Chronic Lymphocytic Lymphoma (CLL) is a heterogeneous disease in which many important factors for its prognosis have been identified. The normal functioning of p53 is one of the most critical barriers against cancer; therefore, if it has a deletion and/or mutation, it is a robust biomarker for the therapeutic response in CLL. The possibility was raised that some germline single - nucleotide polymorphisms of TP53 in healthy populations may also affect p53 function. One of the most studied polymorphisms of the TP53 gene is codon 72 in exon 4, a CGC to CCC transition (R72P), due to its potential effect on cancer risk. As with many types of cancer, its association with a worse prognosis in CLL is unclear. We analyzed the relationship of the genotypes of the TP53 codon 72 polymorphism in a large cohort of patients with CLL, to demonstrate the association of codon 72 with the evolution of the disease.
Using the IDIPHIM patient database, 558 patients with a diagnosis of CLL were included, with clinical data, immunophenotype studies, FISH, IgHV, and karyotype, at the time of diagnosis and during follow-up. The TP53 codon 72 Arg/Arg, Arg/Pro, and Pro/Pro genotypes were analyzed using RT-PCR and Sanger sequencing techniques.
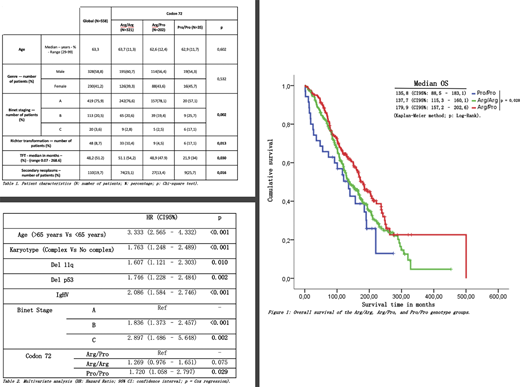
After analyzing the sample of patients, 321 patients with the Arg/Arg genotype, 202 with the Arg/Pro genotype, and 35 with the Pro/Pro genotype were found. In the comparative analysis of the three groups, the patients with the Pro/Pro genotype had a higher number of patients in advanced stages B and C. The latter had a significant association with Binet staging (p = 0.002) compared to the other groups. Likewise, patients with the Pro/Pro genotype had a higher incidence of Richter transformation, whose association was significant (p = 0.013). Also, the patients who were within the Pro/Pro genotype group showed a significant association (p = 0.030) with the Time to the first treatment (TFT), also observing that the group of patients with the Arg/Pro genotype had a more considerable time until your first treatment. 19.7% (110/558) had a second neoplasm, having a significantly higher association with the homozygous groups (Arg/Arg and Pro/Pro) than with the Arg/Pro group, which on the contrary, had fewer second neoplasms (p = 0.016) (see Table 1). Regarding the type of tumors, we found 14.5% of the bladder, 14.5% of the skin, 14.5% of the colon, 13.6% of the prostate, and 12.7% of the lung. No associations were found between Codon 72 and CD38+, ZAP70+, complex karyotype, IgHV, NOTCH-1, del 11q, 12+, p53, del 13q, TP53 mutation. Still, when forming a group between the p53 deletion and TP53 mutation, if significant differences were found (p = 0.023), Pro / Pro group had the highest percentage. The overall survival was 156.32 months (139.92 - 172.72), showing that patients with the Arg/Pro genotype live 40 months more significantly than the other groups (p = 0.028) (see Figure 1). Finally, in the multivariate analysis, age, complex karyotype, 11q deletion, p53 deletion, unmutated IgHV, and Pro/Pro genotype at codon 72 were identified as independent variables associated with an increased risk of death (see Table 2).
In conclusion, the Pro/Pro genotype of TP53 Codon 72 has a potential role in the progression and the higher mortality of patients with CLL. Conversely, the Arg / Pro genotype was associated with a lower incidence of second malignancies and higher overall survival.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal